ENDODONTIC RESEARCH LABORATORY
External and Internal Anatomy of Mandibular Canines with two roots
Anatomia interna e externa dos caninos inferiores com duas raízes
An elective study presented to the Faculty of Dentistry-University of Birmingham for the Degree of Bachelor of Dental Surgery.
As early as 1844 researchers were beginning to investigate tooth anatomy, at which time Carabelli employed simple methods of direct observation to study human teeth. He provided the most detailed description of the root canals (i.e. number and course) prior to 1891. In 1902 GV Black emphasized the importance of the acquirement of knowledge of the details of specific forms of human teeth. Since Blacks time extensive research has been ` carried out in the field of dental anatomy. In 1901 novel methods were being utilized to investigate internal tooth anatomy. Preiswerk injected molten Wood's metal into root canals to analyze the presence of lateral canals and anastomoses in mesio-buccal roots of upper molars and mesial roots of lower molars.
Fisher (1907) used celluloid acetone instead of molten Wood´s metal followed by decalcification.
Grove (1916) injected vulcanite into the canals and decalcified using 5 % nitric acid and rendered the teeth transparent using glycerin.
Callahan (1916) reiterated the importance of knowledge of internal anatomy and in 1917 Hess used the decalcification and diaphanization technique to study internal anatomy and drew several conclusions from his findings. He found that 1.6% of mandibular canines examined, presented with two roots.
Interestingly enough in 1993 Matzer found in his research concerning the anatomy of teeth of Maiz Indians of Guatemala Republic, that the incidence of two rooted canines was as much as 4.1%.
Pineda
and Kutler (1972) categorized the methods used by various researchers as
follows: Direct observation with the aid of a microscope, macroscopic section,
microscopic section, transverse sections and micrometric measurements,
examination of intraoral radiographs, filling and decalcification, filling
and clearing and finally grinding and radiography.
And
so the number of methods possible for the study of tooth anatomy increases
as researchers continually investigate new techniques and modify the old.
We now recognize that for each group of teeth numerous variations of external
and internal anatomy may be observed. It has become evident that the internal
anatomy of root canals does not reproduce the simplicity of the external
anatomy of the tooth.
Why has it become so important to scrutinize the macroscopic appearance of individual teeth Black (1902) believed it necessary to provide a systematized nomenclature of the several parts of the tooth in detail.
However, since the advent of endodontic therapy it has become mandatory to recognize the possible permutations of internal canular morphology in order to provide road maps to successful endodontics. The main objective of endodontic therapy is the thorough mechanical and chemical cleaning of the entire pulp cavity and its complete obtrusion with an inert filling material.
In todays climate of affairs the medico-legal consequences of poor endodontics must be bourne in the forefront of the proffessionals mind. It has become increasingly more important to prolong the life of the natural dentition using conservative methods to retain the correct occluso-vertical dimension for preservation of pleasing facial aesthetics.
Several researchers have investigated failure of root canal therapy due to lack of knowledge of both external and internal tooth anatomy.
In 1982 Robertson and Leeb described the use of the diaphanization method to determine the quality of obtrusion based on the physical appearance of the fill. His experimental method was aimed at being able to visualise the result of instrumentation and obtrusion, in-situ, to provide a mechanism to evaluate endodontic filling techniques, and also to allow a critical self evaluation of practical ability. These methods also provide an insight into possible deviations from the norm which must always be anticipated. For example, Pécora et al (1993) presented a case of endodontic conservative treatment of a maxillary incisor with an atypical crown and type III dens invaginatus. It was found that the root canals were difficult to locate due to the atypical internal anatomy and thus similarly, a tooth with a normal crown appearance may present with aberrations in root morphology.
Ferraz and Pécora (1992) also investigated racial variations in root anatomy which can lead to therapeutic failure if not recognised. Racial anatomic variations have also been demonstrated by Souza-Freitas et al (1971) and Trope et al (1986).
Hence it follows that the use of transparent teeth is indicated in the study of canal anatomy, the teaching of instrumentation and obtrusion techniques and facilitates the learning of endodontic methods, clarifying technical errors not evident clinically.
Glass tubes have been used as transparent root canals, however there is no similarity between the surface of the tubes and the contours of the prepared teeth. The clearing technique gives a three dimensional view of the pulp cavity in relation to the exterior of the tooth. Pao et al (1984) explored the use of computer graphics as an aid to teaching dental anatomy, particularly with respect to the relationship between the pulp and the external tooth morphology in various planes.
A
knowledge of the variations in the anatomy of two rooted mandibular canines
as observed in this investigation, will assist the dentist in reaching
conclusions when diagnosing and treating endodontic cases of these teeth.
Maxillary Molars
Weine (1982) has stated that the frequent failure of endodontic treatment of maxillary molars is likely due to failure to locate and fill the second mesiobuccal root canal, principally in the first permanent maxillary molar.
Hess (1925), Okumura (1927), Pucci and Reig (1944), Pineda (1973), De Oeus (1986); Silveira and Soares (1983), Neaverth et al (1987) have reported the existence of two canals in the mesiobuccal root.
Pécora et al (1992) studied the internal anatomy of three hundred and seventy (370) decalcified and cleared human maxillary molars. The authors observed that 25% of first molars, 42% of the second molars and 36% of third molars studied, presented with four root canals. They observed that the incidence of two root canals in the mesiobnccal root was higher in second maxillary molars than in first molars.
Maxillary
Premolars
First
In order to perform endodontic treatment skillfully and effectively, It is imperative tl; the dentist know tooth anatomy, particularly the internal anatomy.
A lack of knowledge of internal anatomy and its variations will undoubtedly lead to an error in localization, instrumentation and obtrusion of root canals.
Before initiating endodontic treatment, the dentist ought to routinely take two or three radiographs, each at a different angle, to show the exact anatomic variations.
The internal anatomy of the maxillary premolars is particulary complex due to their variation in number of roots and canal configurations.
Several researchers have reported a low incidence of maxillary first premolars with a single canal (Okumura, 1927; Green, 1973; Vertucci and Gegauf, 1979; Bellizzi and Hartwell, 1985).
Hess (1925), Barrett (1925), Pineda and Kutler (1972) and Walker (1987) observed an incidence of a single canal above 10%.
The presence of three canals in the first premolars is relatively low; 35 were found by Bellizzi and Hartwell (1985), none were found by Okumura (1927), Green (1973) and Walker and Quackenbush (1985).
Pécora et al (1991) studied the external and internal anatomy of 240 extracted maxillary first premolars. The external anatomy was studied by measuring each tooth and by observing the direction of the root curvature from the facial and proximal aspects. The internal anatomy of the pulp cavity was studied by a method of making the teeth transparent. A total of 55.8% of the teeth had a single root, 41.7% had two roots and 2.5% had three roots. Consíderíng all of the first premolars studied, the authors found 17.1% had one canal, 80.4% had two canals and 2.5% had three canals.
The discrepancy in a larger number of multiple canals that are found could be due to Various factors, such as; great antomical variation of these teeth, methods used and racial differences.
In the past, many dentists have treated maxillary first premolars assuming them to have just two canals. This should change because we now know that between 0.5% and 7.5% of these teeth have three canals ( Hess, 1925; Barrett, 1925; Pucci and Reig, 1944; Pineda and Kutler, 1972; Carns and Skidmore, 1973; Vertucci and Gegauf, 1979; Bellizzi and Hartwell, 1985; De Deus, 1986; Pécora et al, 1991). Despite the low incidence of three canals, the possibility cannot be overlooked.
Maxillary
Premolars
Second
Pineda and Kutler (1972), Green (1973) did not fmd maxillary second premolars with three canals, however; Hess (1925), Vertucci and Gegauff (1979), Bellizzi and Hartwell (1985), De Deus (1986) and Pécora et al. (1992), all did.
Pécora et al (1992) studied "in vitro" the internal anatomy of 300 maxillary second premolars and observed that one canal was found ín 67.3% two canals in 32.4% and three canals in 0.3%. A total of 90.3% had one root and 9.7% two roots. The direction of curvature was predominantly distal in maxillary sccond premolars with both one or two roots.
MaxiIlary Anterior Teeth.
Maxillary canínes are the largest teeth of the human dentition. ln spite of theìr measurements these teeth present difficulties in radiographic examination. The maxillar canines frequently present with a single root.
The region of the maxillary incisors corresponds to an area of embryological risk, presenting a variety of malformations: Cleft lips, supernumerary teeth, peg shaped teeth, shovel shaped teeth, dens invaginatus and talon cusps.
Pécora et al (1992) published a case report about dens invaginatus in a maxillary canine and Pécora et al (1993) related a case of endodontic conservative treatment ~f a maxillary central incisor with an atypical crown and type III dens invaginatus..
Pécora and Cruz Filho (1992) investigated the incidence of radicular grooves in the upper incisors of 642 patients. Radicular grooves present in 3.9% of the patients, were found mainly on the lingual surface of the maxillary lateral incisor (3.0%). The maxillary central incisor showed radicular grooves on both the buccal and lingual surfàces with an incidence of 0.9%. It was not possible to relate the incidence of these grooves with race (white and negro) or sex.
Pécora et al (1993) presented a case report of a maxillary lateral incisors as teeth with one root and one root canal in 100% of cases (Pucci and Reig, 1944; Ingle and Beveridge, 1976; Weine, 1982; De Deus, 1992). However, this is not always true as several authors have published cases of maxillary lateral incisors with two roots (Swazey, 1888; Madeira, 1973; Christie et al, 1981; Moraes, 1983; Zillich et al. 1983: Thompson et al 19R5: Fahra-Campos, 1990; Pécora and Santana, 1 991).
Mandibular Molars
Three-rooted mandibular molars may be observed in patients of mongolian, caucasian and negro origin. Pucci and Reig (1944) verified an incidence of 5.5% of mandibular molars with three roots in a sample of teeth &om the population of Uruguay.
De Deus (1960) reports an incidence of 2.5% of molars with three roots in a sample of teeth from patients in the Southeast of Brazil. Teixeira (1963), citing an incidence of 10%, reported this extra-root to be smaller than normal roots in the disto-lingual position.
Souza-Freitas et al (1971) using radiographic examination, observed a presence of 17.8% of mandibular first molars with three roots in patients of Japanese descent and only 4.3% in patients of European descent.
Ferraz and Pécora (1992) using radiographic examination of 105 patients of mongolian origin, 106 of negro origin and 117 of caucasian origin observed that the mongolian race showed a greater incidence of three rooted mandibular molars ( 1. mongolian patients, 7.5% of the negro patients and 6.8% of caucasian patients).
The authors did not fmd a statistically significant difference with respect to sex and incidence of this extra-root.
According to literature reviews, a high incidence of mandibular molars with three roots was found in people of mongolian origin (Japanese, Malaysian, Chinese, Thai, Eskimo, Aleutan, American indian) Tratman (1938), Reichart and Metath (1981), Walker and Quakenbush (1985).
Several
researchers have studied the internal anatomy of mandibular premolars (Pineda
and Kutler, 1972; Green, 1973; Vertucci, 1984; DeDeus, 1986; Pécora
et al, 1991). Pécora et al (1991) studied the internal anatomy of
mandibular premolars by the decalcification-diaphanization technique, and
it was observed that 27.45% of the first mandibular premolars presented
with two canals (22.3% with two canals and two foramina and 5.12% with
two canals and one foramina). Only 9.7% of second mandibular premolars
analysed, presented with two canals (5.3% with two canals and two foramina
and 4.4% with two canals and one foramina). The incidence of three canals
with three foramina was significantly low (0.46%) in both first and second
premolars. With respect to mandibular premolar length, the first premolars
presented a maximum value of 26.8 millimetres, a minimum of 18.1 millimetres
and an average of 21.5 millimetres. The second mandibular premolars presented
a maximum value of 27.7 millimetres, a minimum value of 16.1 millimetres
and an average of 22.0 millimetres.
Pécora
et al (1990) studied, in vitro, the incidence of two root canals in the
human permanent mandibular incisors. A total of 634 teeth were analysed,
300 of which were lower central incisors and 334 lower lateral incisors.
The internal anatomy of the root canal was complex because of the high
&equency of double canals with 29.7% in the central incisor and 90.9%
in the lateral incisor. The presence of two canals and two foramina was
2.3% in the lower central incisor and 1.5% in the lower lateral incisor.
The internal anatomy of roots often does not reproduce the simplicity of the external anatomy of the tooth and human mandibular canines do not escape from the rule. They do not present an internal anatomy as simple as could be expected, as demonstrated in cases in which a single root and two canals are present (Barrett, 1925; Pucci and Reig, 1944; Madeira et al, 1973; De Deus, 1992). Cases in which there are two roots have been related (Vanwter, 1886; Taylor, 1886; Koskins, 1923; Hetem et al, 1965; Madeira et al, 1973; DeDeus, 1992; Pécora et al 1993).
Clinicians and endodontists ought to be aware of the existence of mandibular canines with more than one root canal in order to avoid failure during treatment. In fact, failure to localize a possibly existant second canal in mandibular canines generally leads to therapeutic failure due to lack of instrumentation and sealing.
Pécora et al (1993) studied the internal anatomy, direction, number of roots and size of 830 extracted human mandibular canines. The internal anatomy was studied using the methyl salicylate clearing method which showed that 98.3% of these teeth presented with a single root, 92.2% presenting with one canal and one foramina, 4.9% with two canals and one foramen, and 1.2% with two canals and two foramina. The incidence of two-rooted canines was as low as 1.7%. As for the direction of the roots, 5.1 % were straight, 14.6% were mesial, 25.5% distal, 1.0% lingual, 3.2% buccal and 4.4% had sigmoid curvatures. The mean length of the teeth was 25.5 millimetres, with lengths ranging from 20.3 to 32.8 millimetres.
This
literary review shows that mandibular canines with two roots have a low
incidence. The purpose of this research is to investigate the external
and internal anatomy of extracted human mandibular canines with two roots.
Detailed studies have been conducted on all teeth of the maxillary and mandibular arches, however, only a brief review of two rooted mandibular canines has been provided by several workers between 1886 and 1993. Hence in this study the author proposes to investigate only those extracted human mandibular canines that have two roots.
The following items will be observed:
1°
External anaton of teeth. 2° Length of teeth
3°
Root size
4°
Direction of roots
4°
Position of bifurcation
6°
Internal anatomy with particu -ence to the presence of lateral canals
A total of 65 mandibular canines with two roots where studied. The teeth had becn extracted for various reasons and no note was made of patients age, sex or race. Fifty-eight teeth were collected over a period of five years in Ribeirão Preto, Brazil and seven in Birmingham,U.K.
The teeth were cleaned using a curette to remove all traces of hard and solt tissue and then placed in a solution of 5% sodium hypochlorite for approximately one day. Following the cleaning procedure. the topographic dimensions of the teeth were observed and recorded.
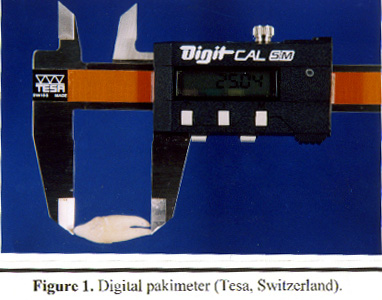
The teeth were measured using a digital pakimeter (Tesa, Switzerland) from the cusp tip to the apex of the buccal root and from the cusp tip to the apex of the lingual root (Figure 1 ).
The direction of root curvature, region of root bifurcation and root size were observed.
The internal anatomy was studied as follows: The mandibular canines were prepared for surgical access to the pulp chamber according to established endodontic procedures. A round diamond bur with a size proportional to the crown was used in the high speed hand piece. Buccal and lingual canals were located using a Maillefer Kerr file (size 10).
The teeth were then immersed in a 5% sodium hypochlorite solution and submitted to a vacuum of 27Kg/cm for 1 hour. The teeth were kept in this solution for three days, thus the remaining pulp tissue was dissolved by a chemical action.
The
teeth were then washed in running water for 6 hours after which time they
were
placed
in a container of 5% hydrochloric acid. A magnetic agitator provided constant
agitation until decalcification was complete (Figure
2).
After decalcitication, the teeth were washed in rurmïng water fór 12 hours to remove all of the remaing acid.
The teeth were then dehydrated for 4 hours in successive solutions of alcohol in an ascending sequence of concentrations (75, 85, 96 and 1 00° GL).
After this, the teeth were injected with gelatin coloured with black India Ink via the pulp chamber, until the gelatin flowed out from the apex. To prepare the darkened gelatin 12g of colourless gelatin was dissolved in 200m1 of cold water. The suspension was warmed until total dissolution was achieved, and then 20m1 of india ink was added. Thc resulting product was stored in the refrigerator to gelatinise.
A carpule syringe with fine needle was used to inject the ink into the teeth, taking care not to mark the exterior surface of the tooth. Any excess was scraped off using a scalpel.
The teeth were then placed in absolute alcohol for 4 hours and forty-nine teeth were immersed in methyl salicylate for diaphanization.
Using this method to make each tooth transpa~ent, the internal anatomy (Shown by the coloured gelatin) was easily observed and studied with minute details of canal configurations being made visible. This method was first described by Pécora et al. (1991).
Following decalcification, dehydration and ink injection, twelve teeth were placed in a jar containing 100m1 of Resapol T 208 resin. This jar was then put into a pressure cooker that had been modified specifically for the experiment (Figure 3).
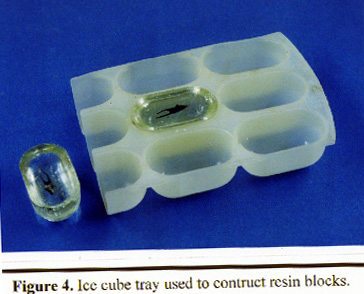
Compressed air was introduced into the pressiuc cooker until a prcssure of 25Lbs per square inch was observed on the manometer. The teeth were maintained in this condition until they were completely diaphanized. Next, two drops of Peroxol catalyst were added to SOmI of the same resin and this solution was placed in each compartment of an ice-cube tray (Figure 4).
A
base was thus prepared by allowing the resin to partially polymcrise in
the pressure cooker again at 25Lbs per square inch of pressure for 12 hours.
The tray was then removed and the teeth were placed on the base. The resin
containing catalyst was added to completely immerse the teeth and the whole
thing placed for the final time into the pressure cooker until the process
of polymerisation was complete i.e. when the resin had changed from the
gelatinous phase to the solid phase. The process was observed at regular
intervals to avoid the formation of bubbles. Any that were formed were
immediately removed using a ball-ended probe. On completion of this process
the blocks of resin were removed from the mould and the transparent teeth
observed at leisure (Pécora et al 1993).
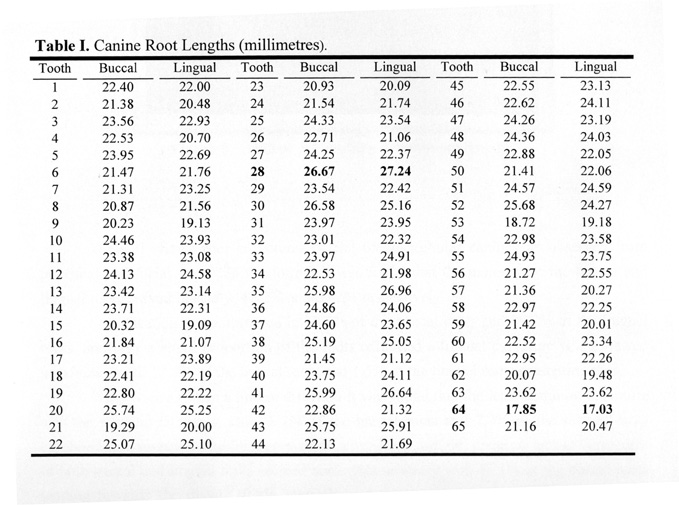
The lengths of the buccal and lingual roots of each tooth was measured and the results tabulated as shown in Table I.
The average length of mandibular canines with two roots as mcasured from the highest point of the crown to the apex of the buccal root and the apex of the lingual root were 22.99 mm and 22.66 mm respectively.
The maximum buccal length was 26.67 mm and the minimum value was 17.85 mm. d the maximuxn lingual length was 27.24 mm and the minimum value was 17.03 mm.
Table I. Canine Root Lengths (millimetres).
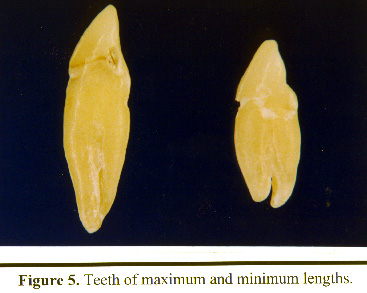
Figure 5 demonstrates the diversity in mandibular canine ,,gest tooth set against the shortest tooth for comparative purposes.
Table II shows root curvatures of the 65 mandibular canines as observed from proximal and facial views. In the former it was found that the majority of the buccal and lingual roots curved buccally, 49.2% and 69.2% respectively.
Straight roots were observed in 38.5% of the buccal roots and 29.2% of the lingual roots, and only a small proportion of the roots exhibited a lingual curvature when viewed proximally with 12.3% of the buccal roots and 1.5% of the lingual roots presenting thus.
When viewed from a buccal direction it was found that the least common curvature was the sigmoid 'S' curve. Only 6.2% of the buccal roots and 7.7% of the lingual roots exhibited this variation.The frequency of occurrence of straight, distal or mesial curvatures of both buccal and lingual roots seemed somewhat arbitrary with 43.1 % of the buccal roots tending towards the distal, 10.8% mesially and the remaining 26% were straight. The lingual root showed only a 1.5% difference in the relative frequencies of curvatures in straight, distal and mesial directions. The actual percentages were 29.2%, 30.8% and 32.3% respectively.
Table II. Direction of root curvatures of 65 mandibular canines with two roots
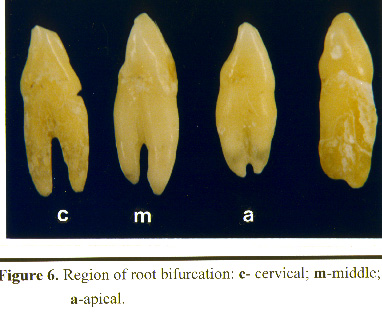
There was found to be a relatively noticeable variation in region of bifurcation of the two rooted canines. An apical bifurcation was seen in 56.9% of teeth, 40% presented with a bifixrcation in the middle third and only 3.1 % in the cervical third (Table III).
Table III. Position of the bifurcation in mandibular canines with two roots.
Figure 6 shows the teeth with root bifurcations in each third, namely; cervical, middle and apical.
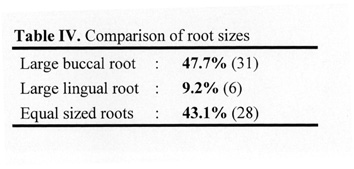
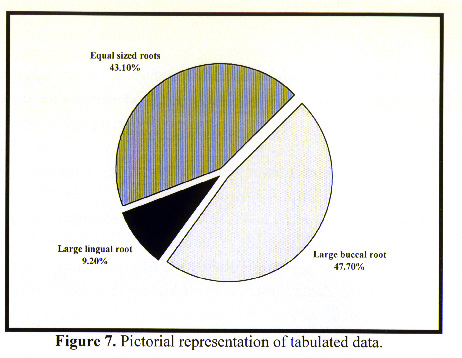
On examination of the size of each root it was observed that the buccal root was the larger of the two in 47.7% of the teeth, and 43.1% had equal sized roots. A larger lingual root was uncommon with as few as 9.2% presenting as such (Table IV).
Table IV. Comparison of root sizes Large buccal root . 47.7% (31), Large lingual root : 9.2% (6) Equal sized roots . 43.1% (28)
The
results of the above table may be better illustrated in the form of a pie
chart
(Figure
7)
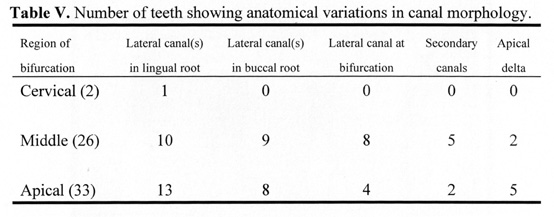
The internal antomy of 61 two rooted mamdibular canines was studied. 1'hc tccth were categorised according to the region of the bifurcation and the frequency of occturence of various features within each group was recorded as shown in Table V.
All teeth examined presented with two root canals. None were observed to have three canals. A number of teeth presented with more than one of the listed anatomical features.
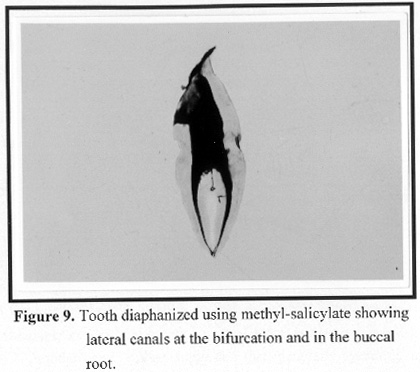
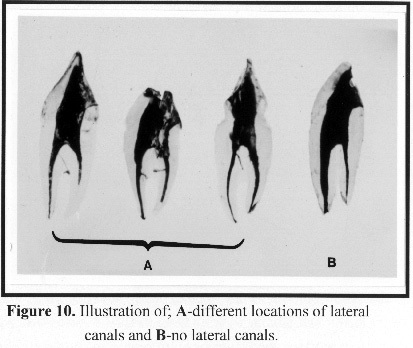
Lateral canals were seen in a total of 68.9% of the teeth whether they extended from the lingual canal, buccal canal or occurred at the bifucation. Only 11.5% of the teeth presented with an apical delta with the majority occurring in those teeth with an apical bifurcation, and 11.5% of teeth presented with secondary canals, however, in contrast to the apical delta, the majority of the secondary canals occurred in teeth with a middle bifurcation.
Table V. Number of teeth showing anatomical variations in canal morphology.
Figure 9 Tooth diaphanized using methyl-salicylate showing lateral canals at bifurcation and the buccL root.
Figure 10 illustration of different locations of lateral canals
Although the existence of two rooted canines has been recognised since 1886, a detailed study of the anatomy has not been conducted. It has now become necessary to investigate the internal anatomy of such anomalies since working with poor anatomic data reduces endodontic success, and thus increases the risk of subsequent extraction. It is important to maintain mandibular canines within the arch not only for aesthetic purposes, but also because of their involvement in lateral excursive movements which, in many individuals, is achieved primarily by canine guidance as opposed to group function.
This study shows both lingual and buccal roots of the two rooted canines to be of approximately equal lengths, with the lingual root being only fractionally shorter. In 1902 Black measured the average length of single rooted canines to be 25.6 mm. It follows that two rooted canines are, on average, shorter than single rooted canines. Operators should be familiar with the average length of teeth so that the correct length of instrument may be selected, and the expected working length known if apical perforation is to be avoided.
In 1972 Grondahl and Mithon suggested that, generally speaking, information on the anatomy of the root(s) and the pulp chamber of individual teeth can be obtained by radiographic examination; however, it is important to know which projections are most informative. Because of the position of the teeth in the jaws, the choice of projections and, therefore, the possibilities of obtaining complete information about the anatomy of the teeth are limited.
There was a significant variation in root curvatures which would inevitably undermine the value of clinical radiographic examination. The buccal and lingual curvatures of both buccal and lingual roots would not be identifiable radiographically.
What is seen on intra-oral radiographs is a poor image of the canals because root canals have three-dimensions. This image is deficient since it is impossible to see buccal or lingual curvatures in the bucco-lingual (proximal) aspect and, according to Pucci and Reig (1944), it is in this plane that root canals exhibit the largest number of variants. Fortunately the percentage of teeth with a lingual curvature in this view was relatively low (1.5%). However, it is evident that a significant proportion of the teeth presented with a buccal curvature (49.2%); therefore, this should be anticipated in endodontic therapy.
Generally only cervical and middle thirds of the teeth are clearly visible r radiographically. However, a well defined view of middle and apical thirds of the root is required since bifurcations were seen to occur most commonly in these regions.
Numerous variations in internal anatomy were also observed here. Therefore if this is made apparent radiographically, two rooted canines may be recognised more easily. In 1979 Slowey suggested that a two rooted mandibular canine may be detected by a change in radiographic density.
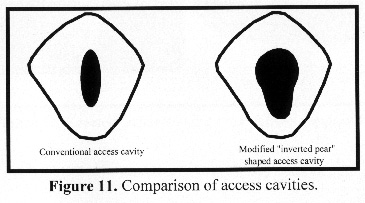
Following the study of the external anatomy, access was gained to the canals. In 1975 Rankine-Wilson stated that the dentist must always be aware of the possibility of a bifurcated root canal in the lower anterior teeth. Single rooted mandibular canines are moderately narrow mesio-distally but very broad bucco-lingually, and a comparable anatomy is observed of two rooted canines. However, the opening must be modified to allow access to the lingual root and canal for adequate instrumentation of the lingual aspect. This is achieved by cutting an "inverted pear" shaped cavity with sufficient lingual extension. The lingual shoulder was removed in a number teeth to gain access to the lingual wall of the root canal. This modification of the conventional access cavity for mandibular canines contraindicates the conservation of the crown substance if failure is to be avoided as a result of insufficient access (Figure 11). Once adequate access had been achieved it was found that curving the instrument slightly allowed the lingual canal to be engaged.
If the access cavity is not prepared correctly then root canal therapy can be frustrating and may be an unsuccessful procedure.
The buccal canal was the one most continuous with the large main passage and therefore was the easiest to instrument. Instrumentation of lingual roots (the narrower of the two in a large proportion of the teeth (see Table IV) and apically bifurcated teeth was decidedly more difficult. With time and patience all teeth were eventually instrumented.
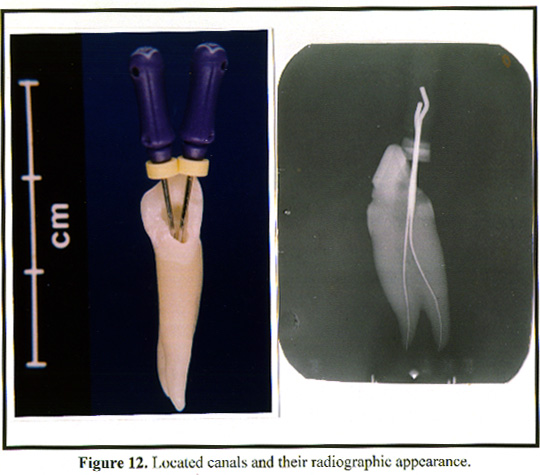
Figure 12 shows that both buccal and lingual canals have been located and the radiographic appearance of the instrumented tooth.
An operator who is oblivious to the presence of a second canal, only enlarges and fills the one most amenable to treatment.
The other is left unfilled. This would explain some of the endodontic failures associated with teeth even though radiographically and clinically the canal systems appear to be obturated.
Figure 13 provides a clear illustration of such a case. A gutta-percha point can be seen in the buccal canal. However, the dentist has failed to observe and hence obturate the lingual canal which has therefore been filled by the ink.
Immersion in 5% soditun hypochlorite solution provides a quick and effective cleaning method. A vacuum is passed through the solution to evacuate the canals of pulp and debris creating patent channels. This method allows preservation of the original mould as emphasised by Prinz in 1913, and is superior to the methods previously used by researchers which involved root canal preparation, obtrusion and finally decalcification.
Decalcification was originally carried out using 5% Nitric acid, however it has since been recognised that the discolouration caused by this acid may be avoided by using a similar concentration of hydrochloric acid. The process is quick, only taking approximately 8-12 hours for each tooth to achieve complete decalcification, with each tooth decalcifying at a different rate.
The teeth may be viewed more clearly using this acid. It is necessary to observe the teeth hourly to avoid total degradation.
Four teeth were lost in this way. The acid is mechanically agitated to avoid incomplete or uneven decalcification. The determination of the end point of this stage of the experiment was simply by examining the flexability of each tooth and listening to the sound when dropped against a laminated surface together with a calcified tooth. Decalcified teeth were flexible and made a dull sound on impact as compared to the sharper sound of the calcified tooth. The teeth were then washed in running water primarily to neutralise the acid.
It is necessary to dehydrate the teeth using ascending concentrations of alcohol so that the process is gradual, and the organic material becomes fixed. Complete dehydration is achieved by keeping the teeth in a solution of alcohol at a concentration of 100%. Opaque patches at sites of incomplete decalcification are thus avoided when teeth are diaphanized.
In 1975 Hasselgren and Tronstad used a contrast medium of water and lndia ink to identify the canals. He found that the ink adhered tenaceously to the root canal walls and was difficult to remove. Incorporation of the ink into gelatin is therefore the optimum method of controlling it. The coloured gelatin flows into all aspects of the canular tree where it is fixed by the alcohol, thus providing a three-dimensional reconstruction of the internal anatomy of root canals.
In 1980 Robertson et al used a method in which the injected ink was drawn through the canal system by applying a negative pressure to the apical end of the tooth with the use of a central suction system. Pécora et al (1993) and the principles adopted in this study utilise no such technique. A positive pressure applied at the pulp chamber automatically forces the gelatin through the canal system. The appearance of a pearl of gelatin at the apex of each canal is a good indicator that the canals have been filled. The lingual canal was difficult to fill in most cases because its narrow diameter offered a greater resistance to the flow of fluid. A similar problem was observed in teeth with apical bifurcations.
Previous authors have used other methods to clarify canal anatomy as mentioned carlier. In 1901 Preiswerk used molten Woods metal but this would not flow into the finer canals and foramina.
In 1907 Fisher used celluloid acetone. This penetrated all foramina of the pulp canals but was brittle and therefore the fine projections or casts of the foramina were easily broken.
In 1925 Hess forced vulcanite rubber into the pulp canals and exposed the casts by dccalcification. Most of the valuable data was gathered using this method.
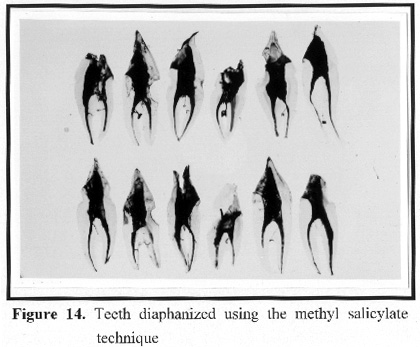
Two techniques of diaphanisation and preservation have been presented. The conventional method involves immersion of the prepared teeth in methyl salycilate. The mandibular canines were rendered totally transparent within five hours. Prinz (1913) described the mechanism of action of this chemical in the diaphanization process. Although very quick and effective, methyl salycilate is potentially toxic and is known to cause nausea, vomiting, acidosis, pulmonary oedema, pneumonia and death. An injection of 30m1 in an adult and lOml in a child is enough to cause death (Merek 1983). The teeth must be kept in a securely closed container, and exposure to the fumes must be minimal, and then only in a well ventilated room. It is vital that the teeth remain in the methyl salicylate solution at all times otherwise the transparency will be permanently reversed and the teeth will become opaque. Hence the time available to carry out a detailed study is limited.
Figure 14 shows the results of this diaphanization technique.
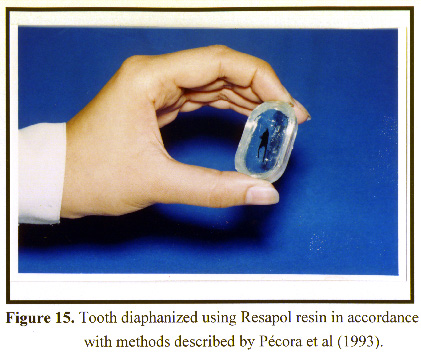
After a period of extensive research, Pécora et al (1993) described a simplified technique for preparing transparent teeth for the study of internal anatomy and their inclusion in resin blocks for permanent transparency. This procedure, although simple, requires more laboratory time because the teeth must be observed at regular intervals to remove newly formed bubbles. In this experiment, only two drops of the catalyst were used (cf three drops used by Pécora et al 1993). This prolonged the polymerisation time with blocks taking at least one week to solidify. However, regardless of the time, this proved to be a more successful method of reducing bubble formation. It was not necessary to polish the blocks which is a very laborious and time consuming process. The blocks may then be manipulated without toxic effects.
Figure 15 show s a tooth diaphanized by this process.
In 1927 Okumura claimed that the trmsparcnt tooth model was the best method because: 1) the original form of the root may be retained; 2) the form of the canal, even its minute structure, can be shown clearly; 3) failure in preparation of the specimen is rare; 4) the specimen can be preserved for a long time (i.e. long shelf life).
This and other methods have produced a mass of statistics illustrating the complexity of the canal system. De Deus (1975) defined a lateral canal as that structure which extends from the main canal to the periodontal ligament, and the secondary canal as the structttre extending from the main canal to the periodontal ligament in the apical region. It was observed that more than 50% of the teeth examined, had lateral canals. This is of some clinical significance since lateral radicular lesions may arise from lateral branchings of'the root canal. In 1963 Nicholls investigated the presence of a lateral radicular lesion associated with a lateral canal and found an association in 4.4% of teeth. The results of this study show that lateral canals occur most frequently in the lingual root. According to Nicholls, successful treatment of the lesion may be achieved by non-sttrgical root canal therapy. However, as stated earlier, the lingual canal was more difficult to instrument. This therefore highlights the clinical implications of endodontic treatment of two rooted mandibular canines. The overall incidence of this anomaly may be very small, but for an operator faced with the treatment of a two-rooted canine, the incidence becomes 100%.
Research such as this raises many questions and opens the door for future work. The author believes that it would be of general interest to investigate the following:
l.
A comparative anthropological study of internal and external anatomy of
teeth from caucasian and asian populations.
2.
An investigative study of cavity design for teeth presenting with anatomical
variations in crown or root morphology.
The results of the former study would be invaluable to the dentist because of the rapid growth of ethnic groups in England.
The latter investigation would help to increase the frequency of successful endodontic treatment of anomalous teeth.
Following the study of the external anatomy of 65 two rooted mandibular canines and internal anatomy of 61 two rootcd mandibular canines, several conclusions may be drawn;
External anatomy:
1
. Two rooted mandibular canines have average buccal and lingual lengths
of 22.99 mm and 22.66 mm respectively.
2.
When viewed proximally, a buccal curvature is most frequently observed
in both buccal and lingual roots
3.
When viewed facially, straight roots arc most frequently observed in the
buccal root and a mesial curvature in the lingual root.
4.
An apical bifurcation is observed most commonly, with a frequency of occurrence
of 56.9%.
5.
The buccal root is the larger of the two in 31 out of 61 teeth (47,&%).
Internal anatomy:
1.
All two rooted mandibular canines have two root canals.
2.
Lateral canals are observed in 68.7% of teeth of which 1 1.5% are furcation
canals.
3.
Furcation canals occur most commonly in teeth in which the root bifurcates
in the middle.
4.
Secondary canals and apical deltas are equally uncommon.
The author studied the external and internal anatomy of human mandibular canine with two roots.
The results of the external anatomy showed that the average buccal root length was 22.99 mm and the average lingual root length was 22.66 mm.
The maximum buccal length was 26.67 mm and the minimiun value was 17.85 mm and the maximum lingual length was 27.24 mm and the minimum was 17.05 mm.
The buccal root was the larger of the two in 47.7% of teeth and 43.1% had equal size roots. The lingual root was larger than the buccal root in 9.2% of cases.
The internal anatomy was studied by decalcification in 5% hydrochloric acid and diaphanization was carried out using methyl salicylate. For identification of the internal anatomy, each tooth was injected with gelatin coloured with India ink.
Diaphanization was also carried out using resin for the construction of resin blocks, allowing permanent preservation.
All mandibular canines with two roots had two root canals. Lateral canals were found in 68.9% of teeth and 19.7% had lateral canals at the bifurcation .
Estudaram-se a anatomia extema e interna de caninos inferiores com duas raízes:.
Os resultados mostraram que o tamanho médio pela vestibular dos caninos foi de 22,99 mm e, por lingual foi de 22.66 mm.
O valor máximo obtido pela face vestibular foi de 26,67 mm, o mínimo foi de 17.85 mm e o valor máximo obtido pela face lingual foi de 27.24 mm e o mínimo foi de 17,03 mm.
O comprimento obtido pela face vestibular foi maior do que o obtido pela lingual em 47,7% dos dentes e, em 43,1% apresentavam-se com valores iguais. O comprimento obtido pela lingual foi maior do que o obtido pela vestibular em 9,2% dos casos.
A anatomia interna foi estudada pelo método da descalcificação em ácido clorídrico a 5% e a diafanização foi realizada com salicilato de metila. Para a identificação da anatomia interna utilizou-se gelatina com tinta da India de cor preta. Usou-se, também, neste trabalho a diafanização com resina para se construir blocos transparentes.
Todos os caninos inferiores com duas raízes apresentaram-se com dois canais. A incidência de canais laterais foi de 68,9% e, na região, da bifurcação encontraram-se canais laterais em 19,7% dos casos.
Barrett MT : The internal antomy of the teeth with special reference to the pulp with its branches . D Cosmos 67:581-592, 1995
Bellizzi R, Hartwell G: Radiographic evaculation of root canal anatomy of in vivo endodontically treated maxillary premolars. J Endodont 11:37-39, 1985
Black GV: Descriptive anatomy of human teeth. SS White Dental Manufacturing Co., Philadelphia 1902
Callahan JR: Multiple apical foramina of tooth roots. J Nat A Ass 3:85, 1916
Carns EJ, Skidmore AE: Configuration and deviations of root canals of maxillary first premolars. Oral Surg 36:880-886, 1973
Carabelli G: Systematisches handbuch der Zahnheilkunde. 2 Vols & Atlas, 8, Wien, 1894, Apud, Hdrlicka A: Shovel-shaped teeth. Am J Phys Anthropol 3:429-465, 1920
Christie WH, Pikoff MD, Acheson DW: Endodontic treatment of two maxillary lateral incisors with anomalous root formation. J Endod 7:528-534, 1981
De Deus QD: Topografia da cavidade pulpar - contribuição ao seu estudo. Doctorate thesis, Belo Horizonte, 1960
De Deus QD: Frequency, location, and direction of the lateral, secondary, and accessory canals. J Endodon 1:361-366, 1975
De Deus QD: Endodontia 4th ed. Medsi, Rio de Janeiro,1986
De Deus QD: Endodontia 5th ed. Medsi, Rio de Janeiro,1992
Fabra Campos H: Failure of endodontic treatment due to a palatal gingival grooves in a maxillary lateral incisor with a talon cusp and two root canals. J. Endodont 16: 342-345, 1990
Ferraz JAB & Pecora JD: Three-rooted mandibular molars in patients of mongolian, caucasian and negro origin. Braz Dent J 3: 113-117, 1992
Fisher G: Uber die feinere anatomie der wurzelkanale menschlicher zahne, deustche monastsch. F Zahnheilk 1907, Apud Mueller A: Anatomy of the root canals of the incisor cuspids and bicuspids of the permanent teeth. J Am Dent Assoc 20: 1365-1386, 1933
Green D: Double canals in single roots. Oral Surg 35: 689-696, 1973
Grondahl HG, Milthon R: Anatomy of roots and pulp cavity - a radiographic and laboratory method of instruction J Dent Educt 36: 30-34, 1972
Grove GJ: The biology of multi canaliculed roots. D Cosmos 58: 728-733, 1916.
Hasseigren and Tronstad: the use of transparent teeth in the teching of preclinical endodontics. J Endodont 1 (8): 24-34, 1975
Hess W: Zur anatomie der wurzelkanale des menschlichen gebisses mit berücksichtigung der feinern verzweigungen am foramen apicale, chweiz. F Zahnheilk 27: 256-260, 1917
Hess W: Anatomy of root canals of the teeth of the permanent dentition. William Wood and Co, New York, 1925
Hetem C, Madeira MC, bernabe JM: Contribuição ao estudo dos caninos inferiores birradiculados. Rev Fac odont Araçatuba 1: 83-92, 1965
Ingle I, Beveridge EE: Endodontics. 2th ed Lea and febiger, Philadelphia 1976
Koskins GA: Cuspids with two roots. D Cosmos 68: 403, 1923
Madeira MC, Hetem C, Tagliavani O, Matheus MTG, Bernabe JM, Marchi F : Canal radicular bifurcado em dente canino inferior: ocorrência e significância clínica. Rev Fac Odont araçatuba 2: 27-30, 1973
Matzer JAC: Anatomia interna e externa dos dentes dos indígenas descendentes dos Maias da república da Guatemala. tese de Mestrado, Ribeirão Preto, 1993
Moraes SH: Incisivo lateral com duas raízes. RGO 31: 108-109, 1983
Nearverth EJ, Kother LM, Kaltenbach RF: Clinicalinvestigation in vivo of endodontically treated maxillary first molars. J Endodont 10: 506-512, 1987
Nicholls I: lateral radicular disease due to lateral branching of the root canal. Oral Surg 16: 839-845, 1963
Okumura T: Anatomy of the root canals J Am Dent Assoc 14: 632-639, 1927
Pao YC, Reinhart RA, Krejci RF, taylor DT: Computer graphic aided instruction of three dimensional dental anatomy. J Dent education 48: 315-317, 1984
Pecora JD, Savioli RN, Murgel CAF: Estudo da incidência de dois canais nos incisivos inferiores humanos. Rev Bras Odont 47: 44-47, 1990
Pecora JD, Saquy PC, Sousa-Neto MD, Woelfel JB: Root form and canal anatomy of maxillary first premolars -Braz Dent J 2: 87-94, 1991
Pecora JD & Santana SVS: Maxillary lateral incisor with two roots. Braz Dent J 2: 151-153, 1991
Pecora JD, Savioli RN, Costa WF, Cruz-Filho AM, Fidel RS: estudo da anatomia interna e do comprimento dos pré-molares inferiores humanos. Rev Bras Odont 48: 31-36, 1991
Pecora JD, Saquy PC, Sousa-Neto MD, Cruz-Filho AM: Morfologia dos dentes humanos anteriores superiores - dimensões, direções das raízes e sistemqa de canais radiculares. Rev inst Cienc Saúde 9: 5-8, 1991
Pecora JD, Woelfel JB, Sousa-Neto MD, Issa EP: Morpholçogic study of the maxillary molars. Part II - internal anatomy. Braz dent J 3: 53-57, 1992
Pecora JD, Cruz-Filho AM: study of the incidence of radicular grooves in maxillary incisor. Braz Dent J 3: 11-16, 1992
Pecora JD, Sousa-Neto MD, Costa WF: Dens invaginatus in a maxillary canine: an anatomic, macroscopic and radiographic study. Australian endodontic Newsletter 18: 12-13, 1992
Pecora JD, Woelfel JB, Sousa-Neto MD, Saquy PC : In vitro study of root canal anatomy of maxillary second premolars 3: 81-85, 1992
Pecora JD, Sousa-Neto MD, Saquy PC. Leite APP: Endodontic treatment of a maxillary incisor with talon cusp - Case report Braz Dent J 4: 127-130, 1993
Pecora JD, Sousa-Neto MD, Saquy PC: Internal anatomy, direction and number of roots and size of humam mandibular canines. Braz dent J 4: 53-57, 1993
Pecora JD, Conrado CA, Zucolotto WG, Sousa-Neto MD, Saquy PC : root canal therapy of an anomalous maxillary central incisor - a case report Endod dent traumatol 9: 260-262, 1993
Pecora JD, silva RS, Sousa-Neto MD: apresentação de uma técnica simplificada de diafanização de dentes e sua inclusão em blocos transparentes. odonto 2: 384-385, 1993
Pineda F, Kutler Y : Mesiodistal and buccolingual roentgenographic investigation of 7275 root canals. Oral Surg 33: 101-110, 1972
Pineda F: Roentgenographic investigation of the mesiobuccal root of the maxillary first molar. Oral Surg 36: 253-260, 1973
Preiswerk G. Die pulpaamputation, eine klinische, pathohistologische and bakteriologische studie. Osterr-ung. V. F. Zahnheilkunde, 1991, v. XVII, P. 145-220, apud, Barret MT:The internal anatomy of the teeth whith special reference to the pulp with its branches. D Cosmos 67: 581-592, 1901
Prinz H: The spalteholz method of preparing transparent animal bodies. Dent Cosmos 55: 374-378, 1913
Pucci FM, Reig R: Conductos radiculares. Barreirros y Ramos, Mondevideo, 1944
Rankine-Wilson RW, Henry P: The bifurcated root canal in lower anterior teeth. J Am Dent Assoc 70:1162-1165, 1975
Reichart PA, Metah D: Three-rootted permanent mandibular first molars in the Thai. Community Dent Oral Epidimiol 9: 191-192, 1981
Robertson D, Leeb J, Mckee M, Brewer E: A clearing technique for the study of root canal systems. J Endodon 6: 421-424, 1980
Robertson D, Leed J: The evaluation of a transparent tooth model system for the evaluation of endodontically filled teeth. J Endodon 8: 317-320, 1982
Silveira NL, Soares IF: Verificação do quarto canal nos primeiro molares superiores permanentes, contribuição ao estudo. Rev Paul Endodont 4: 97-132, 1983
Slowey RR: Root canal anatomy - Road map to sucessful endodontics. Dental Clinical of North America 23: 555-573 1979
Sousa-Freitas JA, Lopes ES, Casati-Alvares L: Anatomy variations of lower first permanent molar roots in two etnic groups. Oral Surg 31: 274-278,1971
Swazey WW: Dental anatomy. D Cosmos 30:372, 1888
Taylor D: Two distinct roots in inferior cuspid. D Cosmos 28: 128, 1886
Teixeira LD: Anatomia dentária humana. Imp Univ Minas Gerais, Belo Horizonte, 1963
Thompson BH, Portell FR, Hartwell GR: Two root canals in a maxillary lateral incisor. J Endodon 11: 353-355, 1985
Tratman EK: Thee-rooted lower molars in man, and their racial distribution. Br Dent J 64: 264-267, 1938
Trope M: mandibular premolars with more than one root canal in different race groups. J Endodon 12: 343-345, 1986
Vanwter GA: Dental anomalies. D Cosmos 28: 64, 1886
Vertucci FJ, Gegauff A: Root canal morphology of the maxillary premolars. J Am Dent Assoc 99: 194-198, 1979
Vertucci FJ: Root canal anatomy of the human permanent teeth. Oral Surg 58: 589- 599, 1984
Walker RT, Quackenbush LE: Three-root lower first permanent molars in Hong-Kong Chinese. Br Dent J 159: 298-299, 1985
Walker RT: Root form and canal anatomy of maxilary first premolares in a Southern Chinese population. Endodont Dent Traumatol 3: 130-134, 1987
Weine FS: Endodontic therapy. Mosby, St. louis 1982
Zillich
RM, Ash JL, Corcoran JF: Maxillary lateral incisor with two roots and dens
formation. A case report. J Endodon 9: 143-144, 1983
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}